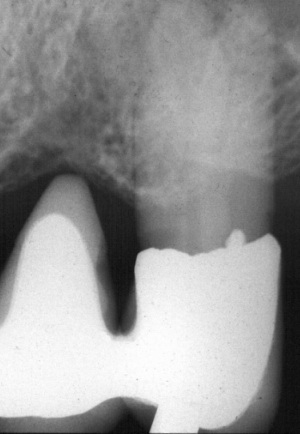
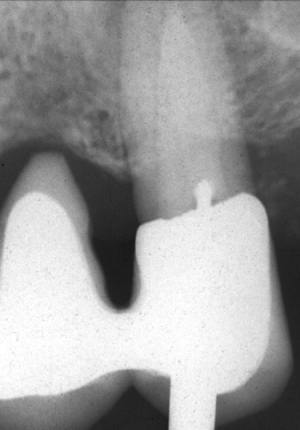
Radiographs indicated that the buccal canal was obliterated coronally. Fiberoptics was used in looking for the canal, but the clinical crown was so long and the crown so narrow that visibility at the cavity floor was not satisfactory. A small, long round bur was then used to penetrate deeper in the root to reach the canal. Frequent radiographic control was employed using mesial and distal projections to quarantee correct direction of the bur.